

Release date:2022-11-22
China is a high-incidence country for gastric cancer, with an estimated annual number of new cases of approximately 679,000 and deaths of approximately 498,000.
Most gastric cancers originate from the mucosal cells inside the gastric wall, known as adenocarcinoma. The gastric wall can be divided into five layers from the inside out: mucosa, submucosa, muscle, subserosa, and serosa. Gastric cancer begins in the innermost layer and grows outward through the gastric wall.
Before gastric cancer occurs, the gastric mucosa often undergoes precancerous lesions. Therefore, correctly addressing and managing precancerous diseases of the stomach is of great significance for reducing the incidence of gastric cancer. Examples include the diagnosis and treatment of Helicobacter pylori infection, the prediction of gastric cancer risk from gastric mucosal atrophy and intestinal metaplasia, and the treatment and evaluation of precancerous lesions. Gastric pepsinogen I and II (PG I, PG II) can indicate gastric mucosal atrophy and have good effectiveness in screening for early gastric cancer in the population.

I. Stomach and Gastric Pepsinogen
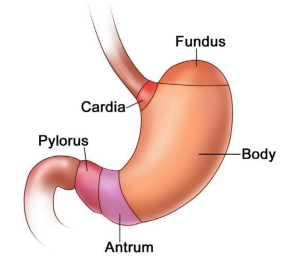
The stomach consists of the cardia, fundus, body, antrum, and pylorus. The body of the stomach is the main part.
Gastric pepsinogen is the precursor of gastric pepsin secreted by gastric mucosal cells, which becomes active pepsin under the action of gastric acid. Gastric pepsinogen (PG) is divided into two subgroups: PG I is synthesized and secreted by the chief cells of the oxyntic glands in the fundus and body of the stomach; PG II can be synthesized and secreted by the oxyntic glands, as well as by the cardiac glands, pyloric glands, and duodenal glands. About 1% of PG can enter the bloodstream through the capillaries of the gastric mucosa, so detecting pepsinogen in the blood serum can reflect the exocrine function of the gastric mucosa.
II. Gastric Pepsinogen and Atrophic Gastritis
Helicobacter pylori is the main cause of chronic gastritis, which can induce the gastric mucosa to secrete more pepsinogen. When the gastric mucosa is inflamed, the levels of PG I and PG II entering the bloodstream increase. As the inflammation progresses and the gastric mucosa atrophies, the number of secretory glands in the stomach body and fundus decreases or is replaced by pyloric glands, leading to a decrease in PG I levels, while the secretion of PG II by secretory cells is more widespread and has less impact, resulting in a gradual decrease in the PG I/II ratio with the severity of gastric body atrophy.
Studies have shown that checking PG I, PG II, and the PG I/II ratio can help diagnose gastric mucosal atrophy. Clinically, PG I ≤ 70 μg/L and PG I/II ≤ 3 are considered positive results, with good screening effects.
III. Gastric Pepsinogen and Gastric Cancer Screening
The "Chinese Consensus on Early Gastric Cancer Screening and Endoscopic Diagnosis and Treatment (April 2014, Changsha)" suggests that the risk of gastric cancer is divided into four levels:
Level A: PG (-) Hp (-), no need for endoscopic examination;
Level B: PG (-) Hp (+), endoscopic examination should be performed at least every 3 years;
Level C: PG (+) Hp (+), endoscopic examination should be performed at least every 2 years;
Level D: PG (+) Hp (-), endoscopic examination should be performed at least every 1 year.
Here, PG (+) refers to PG I ≤ 70 μg/L and PG I/II ≤ 3, and Hp refers to the results of Helicobacter pylori antibody detection.
The risk of gastric cancer in groups A, B, C, and D gradually increases, with groups C and D having a higher incidence of gastric cancer.
This gastric cancer risk classification does not apply to cancer at the gastroesophageal junction (cardia cancer).
References:
[1]Liao Z, Sun T, Wu H, et al. Chinese Consensus on Early Gastric Cancer Screening and Endoscopic Diagnosis and Treatment (April 2014, Changsha)[J]. Gastroenterology, 2014.
[2] National Clinical Research Center for Digestive Diseases, Chinese Society of Digestive Endoscopy, Chinese Society of Health Management, et al. Chinese Consensus on Early Gastric Cancer Screening Process (Draft) (2017, Shanghai)[J]. Chinese Journal of Health Management, 2018(1):8-14.
[3] Ying X, Lv B. Value of Pepsinogen and Gastrin-17 in the Diagnosis of Atrophic Gastritis[J]. Clinical Summaries, 2019, 34(5):4.
[4]Gastroenterology Branch of China Association of Chinese Medicine, Collaborative Group of Chinese Society of Digestive Diseases and Digestive Endoscopy, Collaborative Group of Early Cancer of Chinese Society of Digestive Endoscopy, et al. Clinical Management Guidelines for Integrated Gastric Cancer Precancerous Lesions in China[J]. Chinese Journal of Integrated Traditional and Western Medicine for Digestion, 2022(003):030.

